


Lindsey Vonn is one of the most successful and decorated alpine ski racers in history. She’s dominated international competition for nearly two decades, winning four women’s World Cup titles and Olympic medals, including downhill gold in 2010, before initially retiring in 2019.
Throughout that career, Vonn battled. She suffered multiple anterior cruciate ligament (ACL) tears, knee ligament sprains, tibial plateau fractures, ankle breaks, and a fractured humerus.
Many of these setbacks cost her whole seasons and forced repeated surgeries and rehabilitations.
By the late 2010s, the cumulative toll of these injuries was clear: Vonn once remarked that her body was “broken beyond repair”, prompting her first retirement.
However, after a partial knee replacement in 2024, she returned to racing and became the oldest female downhill winner in World Cup history in 2025.
Comeback and a catastrophic crash
Vonn’s final professional goal was the 2026 Winter Olympics in Milano-Cortina, Italy. Remarkably, she chose to compete despite rupturing her ACL in her left knee at a World Cup race just nine days before the Olympic downhill. She qualified and started the race held on 8 February.
But about 13 seconds into her downhill run she clipped a course marker and crashed violently, leading to multiple severe injuries. First, she sustained a complex tibial fracture at the ankle in her left leg. Shards of her shinbone were broken in multiple places.
Lindsay Vonn’s crash. She has been airlifted to the hospital and her condition is unknown. After a 35 minute delay, racing has started again in the Women’s Olympic downhill. American Breezy Johnson still leads the event. pic.twitter.com/NCp8ZxhUEo
— The Fall Of Rome (@FallofRome) February 8, 2026
But the most dangerous development came shortly after the crash: Vonn’s leg developed acute compartment syndrome (ACS).
“He filleted it open and let it breathe, and he saved me.” – Lindsey Vonn, on her emergency surgery.
Anatomy of an emergency: What is compartment syndrome?
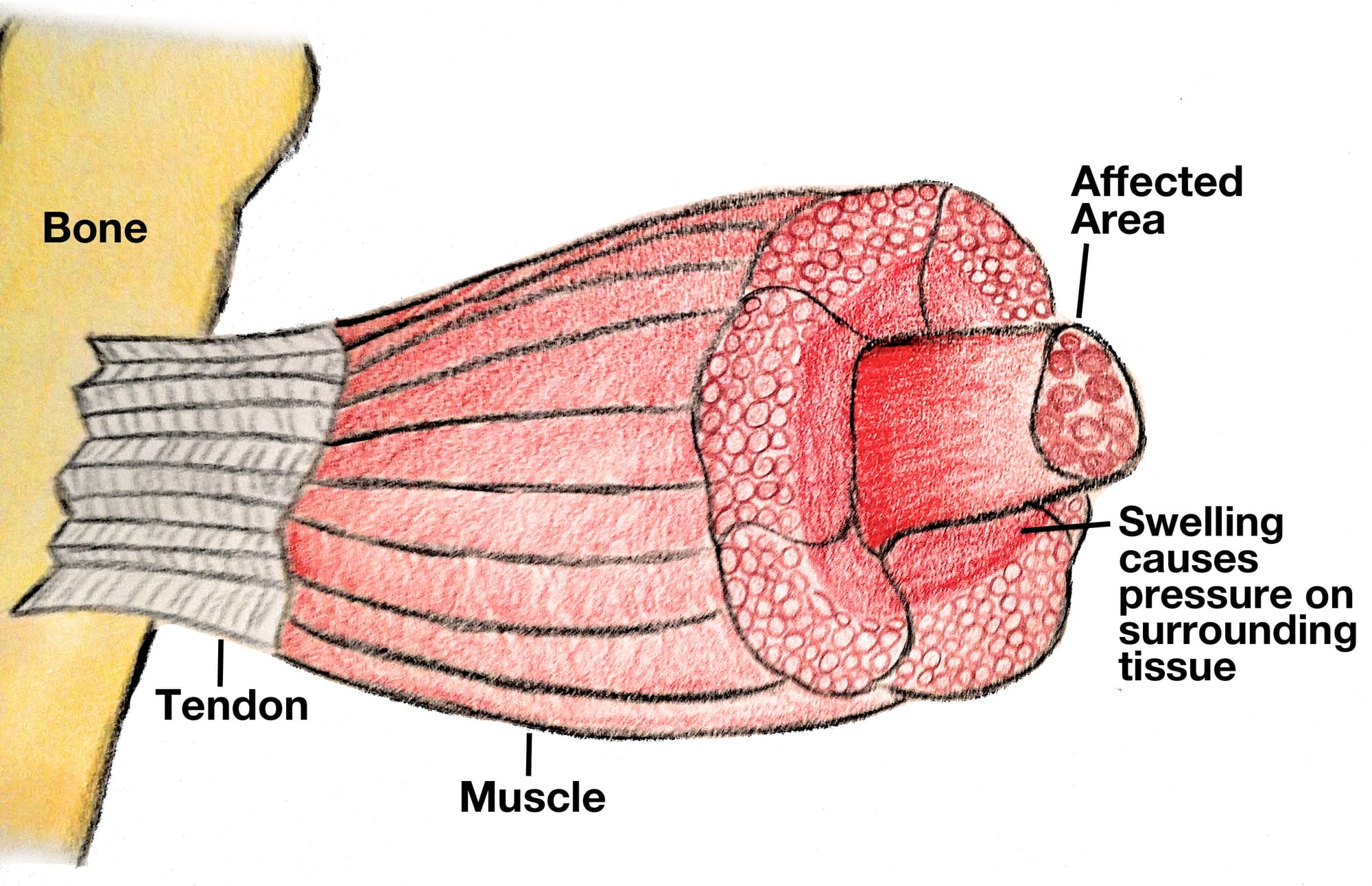
Our limbs are divided into “compartments” – groups of muscles, nerves and blood vessels wrapped in a tough, inelastic sheet of connective tissue called fascia.
While fascia is excellent at keeping structures in place, its lack of “give” is its fatal flaw during trauma. When a high-energy injury occurs – such as Vonn’s tibial fracture – internal bleeding or inflammatory swelling causes the pressure within these tight compartments to skyrocket.
When the compartment pressure exceeds the pressure of the small capillaries supplying the tissue, blood flow stops. The muscles are effectively strangled in their own casing.
As Vonn explained, the build-up of blood oedema, resulting in increased compartment pressure, “basically crushes everything” in the compartment and can endanger the viability of the entire limb.
Without immediate intervention, the lack of blood flow and oxygen can cause muscle, nerve and tissue death, a threat so severe that amputation becomes a real risk.
The clinical ‘red flags’
Early diagnosis is the holy grail of ACS management, yet it’s notoriously difficult. The classic “five Ps” (pain, pallor, pulselessness, paresthesia and paralysis) are often taught, but as a surgeon deciding to operate or not, relying on them can be a fatal mistake.
- Pain out of proportion: This is the earliest and most reliable sign. If a patient’s pain is screaming louder than the visible injury suggests – and is unresponsive to strong opioids – suspicion must be immediate.
- Pain on passive stretch: Stretching the affected muscle group causes excruciating agony.
- Measuring the compartment pressure: When the diagnosis is unclear, surgeons use a specialised needle manometer to measure the pressure directly. If the “Delta pressure” (the difference between the patient's diastolic blood pressure and the compartment pressure) is less than 30mmHg, the limb is in the danger zone.
The cost of a missed diagnosis
A missed diagnosis is catastrophic. Within just six hours of ischemia (lack of oxygen), dead muscle begins to set in.
If the pressure isn’t relieved, the necrotic tissue eventually scars and shrinks, leading to Volkmann’s Contracture. This permanent deformity leaves the limb clawed, stiff and largely non-functional, a haunting legacy of a window of opportunity closed too soon.
Beyond the risk to the limb, ACS can become life-threatening. As muscle cells die, they rupture and leak a protein called myoglobin into the bloodstream, a process known as rhabdomyolysis.
This “cellular debris” can clog the kidneys, leading to acute renal failure and systemic collapse. This is why CK (creatine kinase) monitoring is vital; a spiking CK level is a chemical siren that the body is breaking down from within.
The solution: A multidisciplinary sprint
The only definitive treatment for ACS is an emergency fasciotomy. Surgeons – usually plastic surgeons in Australia – make long, deep incisions through the skin and then the fascia to “unzip” the compartment and allow the swollen muscle to bulge out, immediately restoring blood flow.
Although predominantly an operation carried out by plastic surgeons, in an emergency it can be done by orthopaedic, vascular or general surgeons depending on the geographical setting and services available locally.
There’s no time to transfer the patient – the operation must be carried out before relocating them to a trauma unit.
Because the swelling is so severe, these wounds cannot be closed immediately. They’re often managed with specialised negative-pressure “vacuum” dressings and require a multidisciplinary team (MDT) approach to get the patient healed and back on their feet.
- Orthopaedic surgeons stabilise the broken bones with steel rods, plates and screws or external fixation frames.
- Plastic surgeons manage the complex soft-tissue coverage and eventual skin grafts.
- Intensivists and nurses monitor for systemic complications such as rhabdomyolysis, managing shifts in fluids and electrolytes.
- Physiotherapists begin the gruelling road to reclaiming mobility, and prevent deconditioning of the other limbs.
A lesson in vigilance
Lindsey Vonn’s story ended with her leg intact, thanks to the presence of her lead surgeon and the rapid transition to the operating theatre. But for many, the “hidden” nature of compartment syndrome remains a silent threat.
Vonn’s recent revelation that she nearly lost her leg serves as a visceral reminder of a condition that remains one of the most feared surgical emergencies in medicine. It’s a race against a ticking clock where the prize is limb salvage and, occasionally, life itself.
Clinicians maintain a “high clinical suspicion” for compartment syndrome in trauma patients. In the battle between pressure and perfusion, time isn’t just money, it’s muscle.



